- The paper introduces an innovative Attention-ResUNet architecture that integrates residual learning with multi-scale attention for enhanced fetal head segmentation.
- It achieves a mean Dice coefficient of 99.3%, outperforming standard U-Net variants and demonstrating statistically significant improvements.
- The study validates model robustness and interpretability with Grad-CAM saliency analysis, ensuring reliable deployment in clinical settings.
Attention-ResUNet for Automated Fetal Head Segmentation: Summary and Analysis
Introduction
Accurate segmentation of the fetal head in ultrasound (US) imagery is indispensable for reliable prenatal biometric analysis. Persistent challenges in clinical ultrasonography—such as pronounced speckle noise, low tissue contrast, and ambiguous anatomical boundaries—undermine segmentation accuracy. Canonical architectures like U-Net established the blueprint for biomedical segmentation but remain susceptible to gradient attenuation in deep layers and exhibit indiscriminate feature selection. The presented work proposes the Attention-ResUNet, an architecture that combines residual learning with hierarchical multi-scale attention mechanisms, engineered for robust, interpretable fetal head segmentation in challenging US conditions (2604.18148).
Architectural Innovations
The Attention-ResUNet integrates multi-scale attention gates at four consecutive decoder levels (facilitating 64, 128, 256, 512 channel feature maps) atop an identity-mapping residual U-Net backbone. This configuration ensures both spatially selective gating of salient anatomical structures and uninterrupted gradient flow throughout the network—critically addressing both feature localization and training stability.
Residual blocks reformulate layers into additive mappings F(x)+x, facilitating deep network optimization. Attention gates receive features from both the encoder and current decoder levels, compute spatial attention coefficients via parameterized convolutions, and modulate encoder features, effectively focusing on structurally relevant regions while suppressing background artifacts.
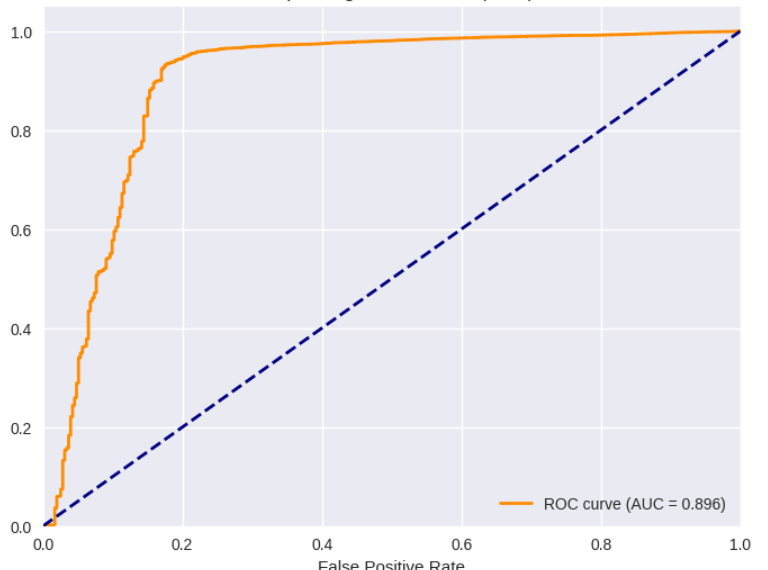
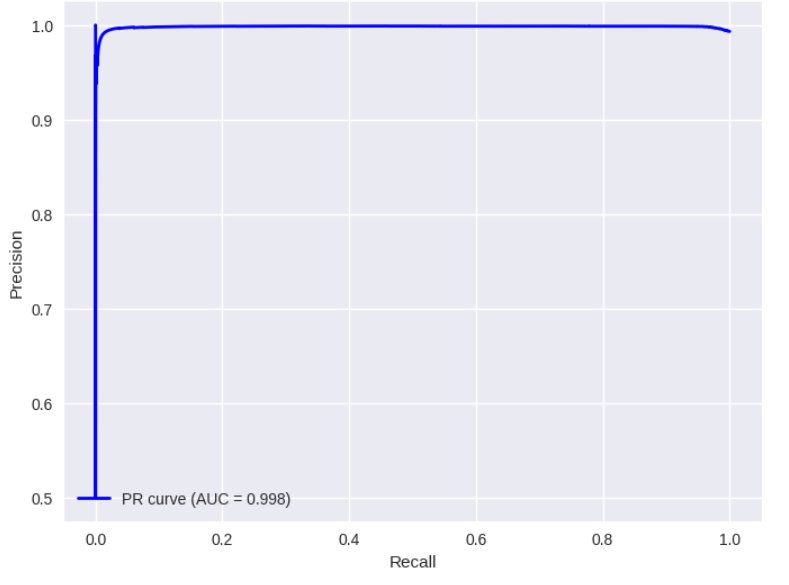
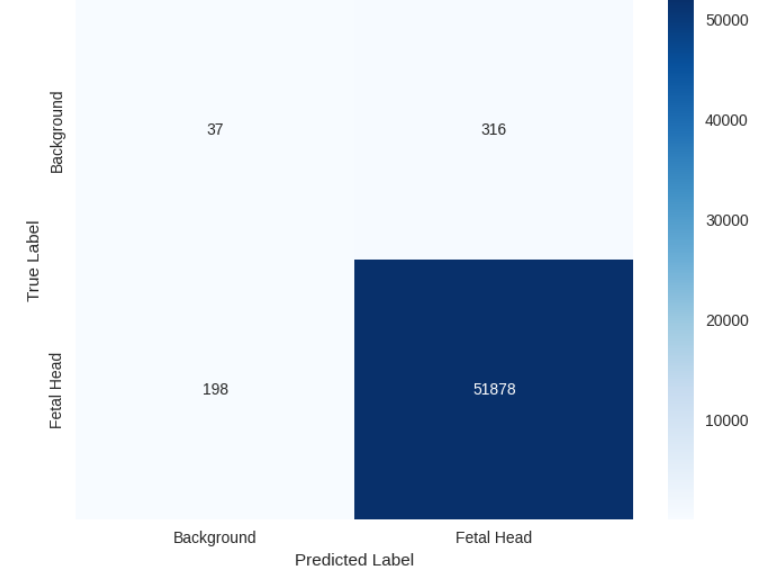
Figure 1: (a) ROC curve, (b) Precision vs Recall curve, and (c) Confusion Matrix for the Attention ResUNet Architecture.
The union of these mechanisms in the proposed U-shaped network allows robust multiscale feature aggregation, with each skip connection passing through an attention gate for context-aware refinement. A final pointwise convolution and sigmoid activation yield the segmentation probability map.
Experimental Setup
Evaluation employed the HC18 Challenge dataset (n=200 for validation), with preprocessing—including intensity normalization, random geometric and photometric augmentation—to emulate real-world clinical image variability. Primary metrics included Dice Similarity Coefficient (DSC), Intersection over Union (IoU), precision, recall, F1-score, Hausdorff Distance (HD), and Average Symmetric Surface Distance (ASD). Optimization utilized Adam (lr=1×10−4), batch normalization, and deterministic training for reproducibility. Baseline comparisons encompassed ResUNet, Attention U-Net, Swin U-Net, standard U-Net, and U-Net++.
Attention-ResUNet achieved a mean Dice of 99.30±0.14%, surpassing all baselines, including ResUNet (99.26%), Attention U-Net (98.79%), Swin U-Net (98.60%), standard U-Net (98.58%), and U-Net++ (97.46%), with all improvements statistically significant (p<0.001; effect sizes n=2000–n=2001). The AUC-ROC was 0.896 and AUC-PR was 0.998, evidencing superior sensitivity, specificity, and precision-recall trade-offs. The confusion matrix highlighted a negligible rate of false negatives.
Boundary metrics further validated the architecture’s efficacy: median HD was 38.0 pixels and median ASD was 13.2 pixels—minimal compared with all comparators.
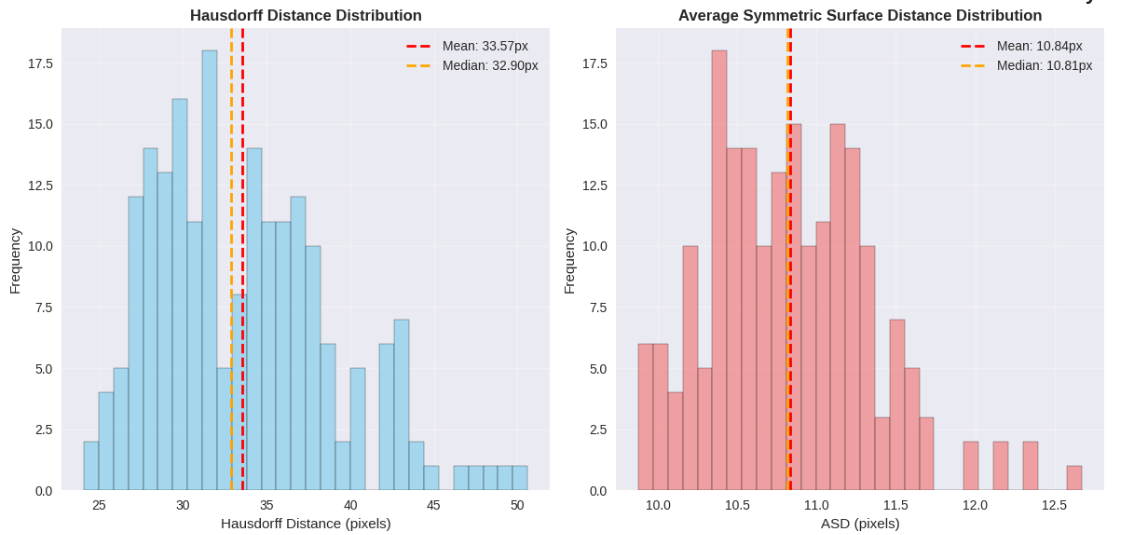
Figure 2: Hausdorff Distance (left) and ASD (right) distributions.
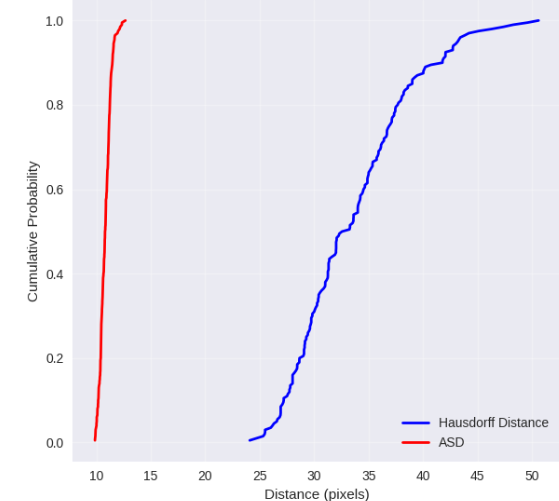
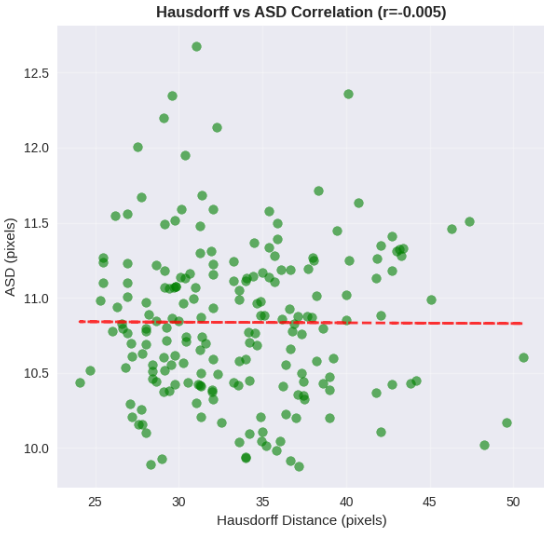
Figure 3: Hausdorff and ASD Distance correlation analysis.
Statistical robustness was systematically established using paired t-tests and confidence intervals; the narrow interquartile ranges in Dice and IoU further reflected high segmentation consistency.
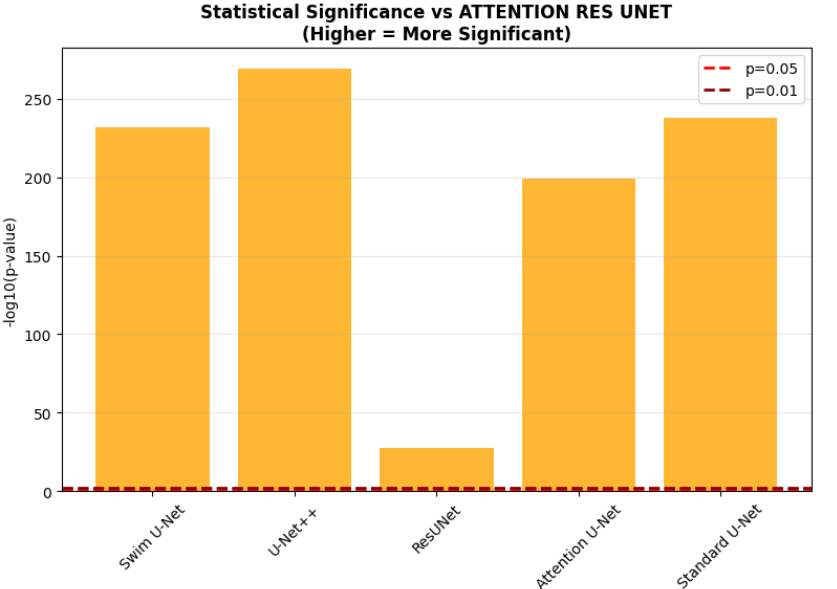
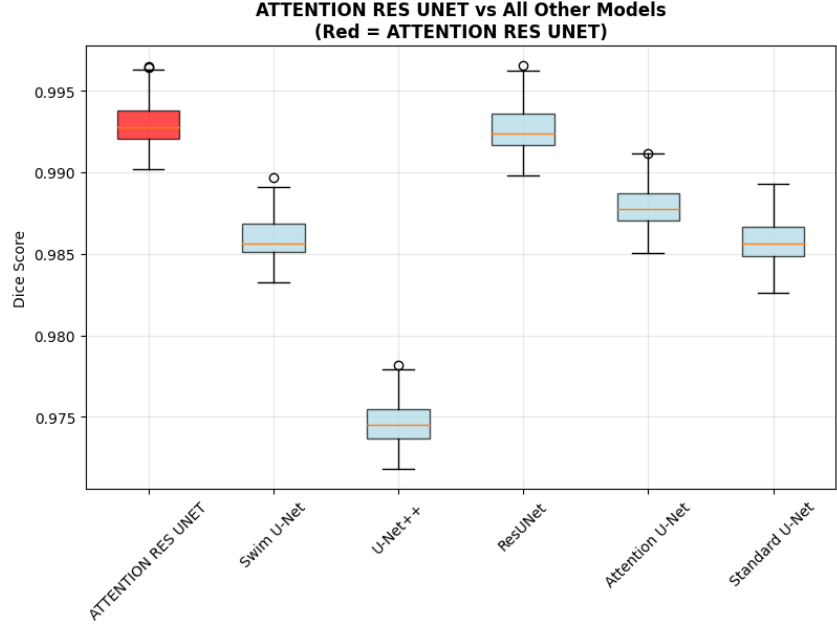
Figure 4: Statistical significance against the proposed model.
Interpretability via Saliency Analysis
Model interpretability was systematically assessed using Grad-CAM-based saliency mapping and comparative visualization across candidate architectures.
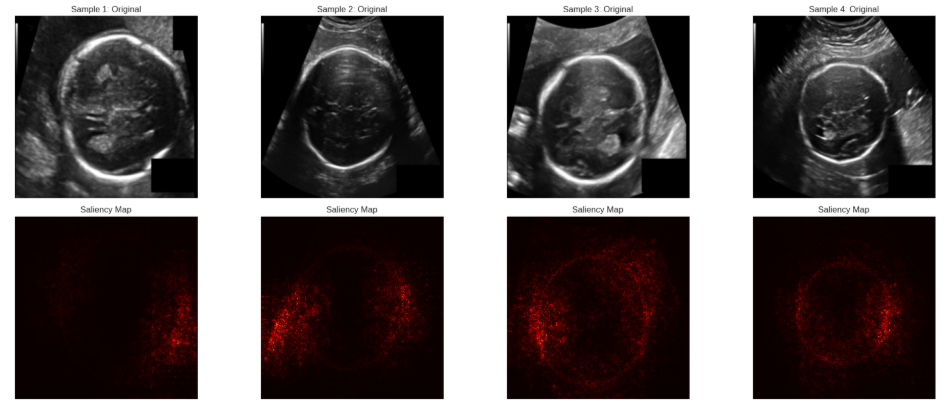
Figure 5: Saliency map with diffuse activation patterns for ResUnet
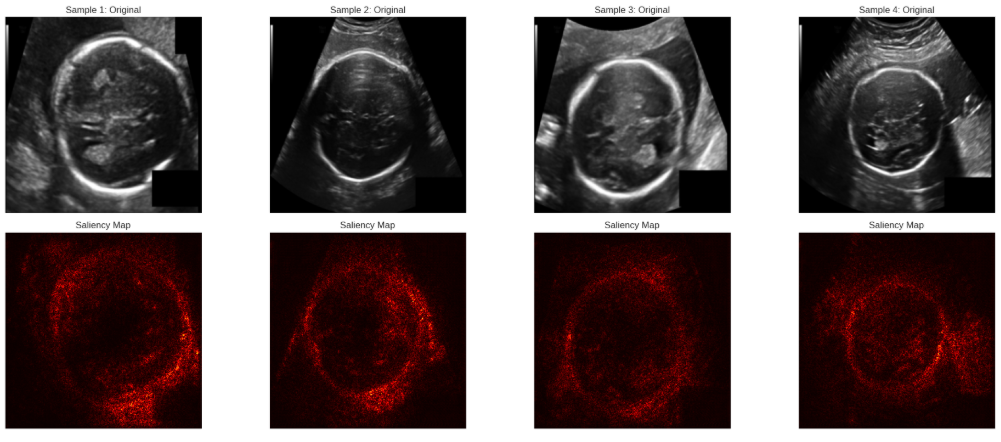
Figure 6: Saliency map showing precise focus on target region via Attention UNet
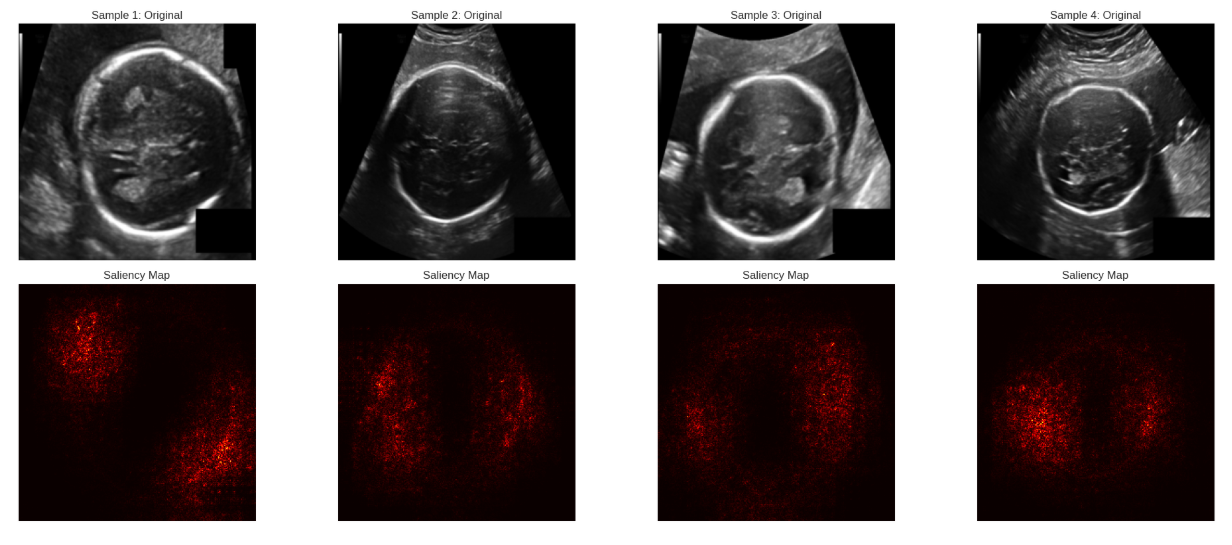
Figure 7: Saliency map showing enhanced spatial precision via Attention ResUNet
ResUNet displayed diffuse activations spanning irrelevant regions. Attention U-Net sharply concentrated activations but occasionally missed structural completeness under challenging cases. Attention-ResUNet consistently yielded focused, anatomically congruent activations—exemplified by the highest spatial concentration index (n=2002, n=2003 vs. all baselines). This indicates that multi-scale attention in conjunction with residual channels materially enhances clinical interpretability and trust.
Computational Considerations
Remarkably, despite architectural complexity, computational efficiency was maintained: 14.7M parameters and 45 GFLOPs per n=2004 slice, delivering 23 ms inference on RTX 3080 hardware. This supports deployment in time-critical clinical workflows without resource constraints.
Limitations and Outlook
Although state-of-the-art performance was conclusively demonstrated on HC18, cross-manufacturer variability and broader clinical acquisition diversity remain untested. Degraded performance was noted under substantial acoustic shadowing (~3–5% scans) and non-standard head planes, with Dice dropping to 97–98%. Future work should prioritize extension to volumetric 3D US, clinical multi-center validation, uncertainty quantification for error-awareness, and domain adaptation for cross-device generalization.
Conclusion
Attention-ResUNet delivers substantial performance gains in automated fetal head segmentation, leveraging the synergy of residual learning and hierarchical attention for robust and interpretable prediction. Both strong statistical evidence and saliency interpretability underscore its readiness for clinical integration—provided prospective validation on broader populations and imaging conditions.
The demonstrated paradigm—residual backbone supporting multi-scale attention refinement—presents a robust template for further research in medical segmentation and other challenging domains where fine-grained, trustworthy localization is essential.

