- The paper introduces a semi-parametric extension to the Cox model to rigorously incorporate right-censored covariates.
- It leverages a weighted averaging method, often using the Kaplan-Meier estimator, to replace the standard relative risk component and reduce bias.
- Simulation studies and clinical applications in oncology data demonstrate improved precision and power compared to complete case analysis.
Advanced Estimation in Cox Models with Right-Censored Covariates
Introduction
The issue of censored covariates in time-to-event analyses is a pervasive challenge in clinical and epidemiological research, particularly in oncology where intermediate outcomes such as progression-free survival (PFS) or time-to-progression (TTP) are hypothesized to predict overall survival (OS). Standard Cox regression accommodates censoring in outcomes but offers little for covariates observed subject to right censoring. Conventional approaches—such as complete case (CC) analysis and constant imputation—are inefficient or biased in these scenarios. The paper "Cox Model Predicting Covariate Subject to Right Censoring" (2604.10088) presents a semi-parametric extension to the Cox proportional hazards model that rigorously incorporates right-censored covariates into estimation, using a data-driven variant of the Innovation Theorem.
Methodological Overview
The proposed method adapts the Cox model's partial likelihood by replacing the relative risk term for censored covariates with a weighted average based on the observed sample. Specifically, if W is a covariate subject to right censoring and T is the survival outcome, the modified relative risk for censored W employs the conditional distribution of W given that its true value exceeds the observed censoring threshold. Weights are determined non-parametrically (typically via the Kaplan-Meier estimator), although stratified or regression-based approaches are also allowed if dependency on fully observed covariates is anticipated.
This innovation permits retention of all individuals in the analysis, improving both efficiency and power relative to CC methods. The likelihood function is then maximized via Newton-Raphson, leveraging gradients and Hessians calculable from the weighted forms.
Simulation Results
Comprehensive simulation studies evaluate bias, empirical standard error, mean squared error (MSE), and coverage probability under multiple settings:
- Scenario 1: Continuous covariate with uniform censoring and multiple observable covariates.
- Scenario 2: Mimics oncology settings by examining surrogacy of PFS for OS, including composite time-to-event endpoints and direct/indirect treatment effects.
- Scenario 3: Explores impact of non-uniform (Weibull) censoring mechanisms on estimator performance.
Across most settings, the proposed estimator provides lower MSE and variance than CC and generally retains nominal coverage rates. Notably, in highly unequal censoring regimes, some underestimation of effect size and coverage erosion are observed if large covariate values are disproportionately censored. This is attributable to the inability to reconstruct likelihood contributions for extreme censored observations, especially when few larger observed covariates are available as reference.
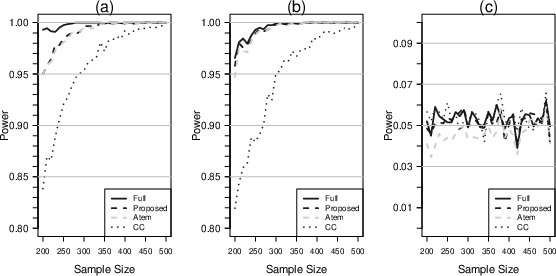
Figure 1: Empirical power for testing null effects on gamma and selected beta coefficients under increasing sample size, demonstrating statistical efficiency of the proposed method over CC.
Application to Clinical Oncology Data
The utility of the method is illustrated on two datasets:
- Prostate Cancer Trial (CHAARTED): Examining whether PFS/TTP predict OS using randomized assignment between androgen deprivation and combination therapy.
- Breast Cancer Cohort (Rotterdam): Assessing if relapse-free and time-to-relapse endpoints provide predictive surrogacy for OS.
In both settings, the authors utilize resampling and permutation to decouple predictive surrogacy from treatment effects, repeatedly estimating the relevant Cox models and comparing the p-value distributions between methods.
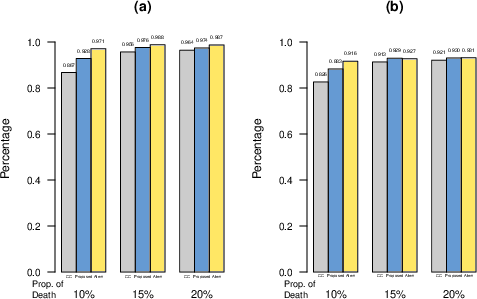
Figure 2: Frequency of statistical significance for intermediate endpoints (e.g., PFS predicting OS) and joint surrogacy conditions across simulation repetitions.
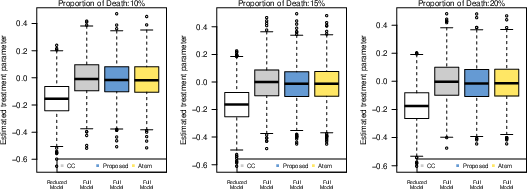
Figure 3: Boxplots of treatment effect estimates for reduced (treatment only) vs. full (treatment and intermediate covariate) Cox models, showing attenuated apparent treatment effect when controlling for the intermediate.
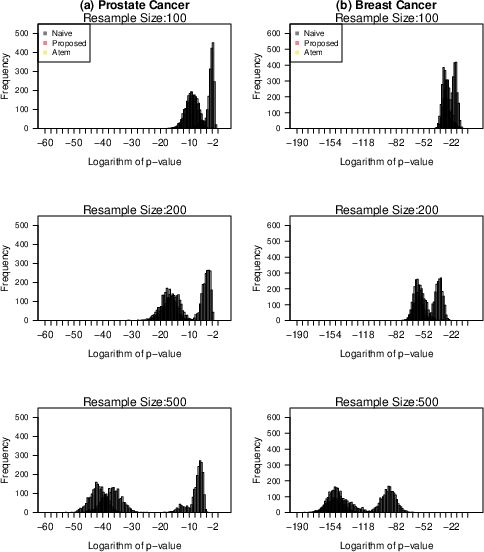
Figure 4: P-value distribution (log scale) for surrogacy assessment in prostate and breast cancer data, comparing the proposed, Atem, and CC approaches.
These empirical analyses confirm that the intermediate time-to-event endpoints are highly predictive of OS, particularly with robust sample sizes and balanced designs. Discrepancies between p-value distributions across estimation strategies further highlight the improved variance estimation with the proposed method.
Theoretical and Practical Implications
The revised partial likelihood fosters improved statistical power for detecting true associations with right-censored covariates, particularly when censoring is not extreme at the covariate distribution's upper end. Compared to existing imputation or expectation-maximization methods, this framework is both computationally efficient and better able to accommodate auxiliary covariate information.
Theoretical implications extend to surrogate endpoint validation, as the approach enables formalization of Prentice-type criteria in the setting where surrogates are themselves censored time-to-event variables. However, bias may arise if censoring is highly unequal or when the conditional support for censored covariates is limited, underlining the need for diagnostic assessment of censoring patterns in practice.
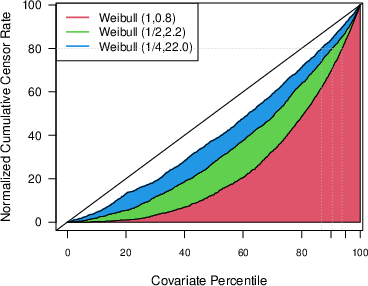
Figure 5: Cumulative covariate censoring rate as a function of empirical percentile under various Weibull parameter regimes, illustrating the influence of censoring mechanism.
Limitations and Recommendations
While the method is broadly applicable to clinical and epidemiological research settings, it assumes sufficient empirical support for the weighted reconstruction of censored covariates. In practice, the presence of heavily censored upper quantiles should prompt caution. The paper recommends routine examination of histograms of observed covariates and scrutiny for discontinuities, as well as cautious interpretation of surrogacy inferences when death is a major component of secondary endpoints.
Conclusion
This work presents an effective and statistically principled approach to Cox model estimation with right-censored covariates. By leveraging weighted averages based on observed data, the method improves statistical precision and power over naïve approaches, facilitates surrogate endpoint assessment, and enables more informative modeling in survival analysis. Nevertheless, performance is intimately tied to censoring patterns, and future methodological developments may further address scenarios with extreme or non-ignorable censoring and extend the approach to non-proportional hazards or time-varying covariate structures.

